Feline Lower Airway Disease with Tree-in-Bud Appearance on Radiographs and Computed Tomography
Diagnostic Imaging

SIGNALMENT AND HISTORY
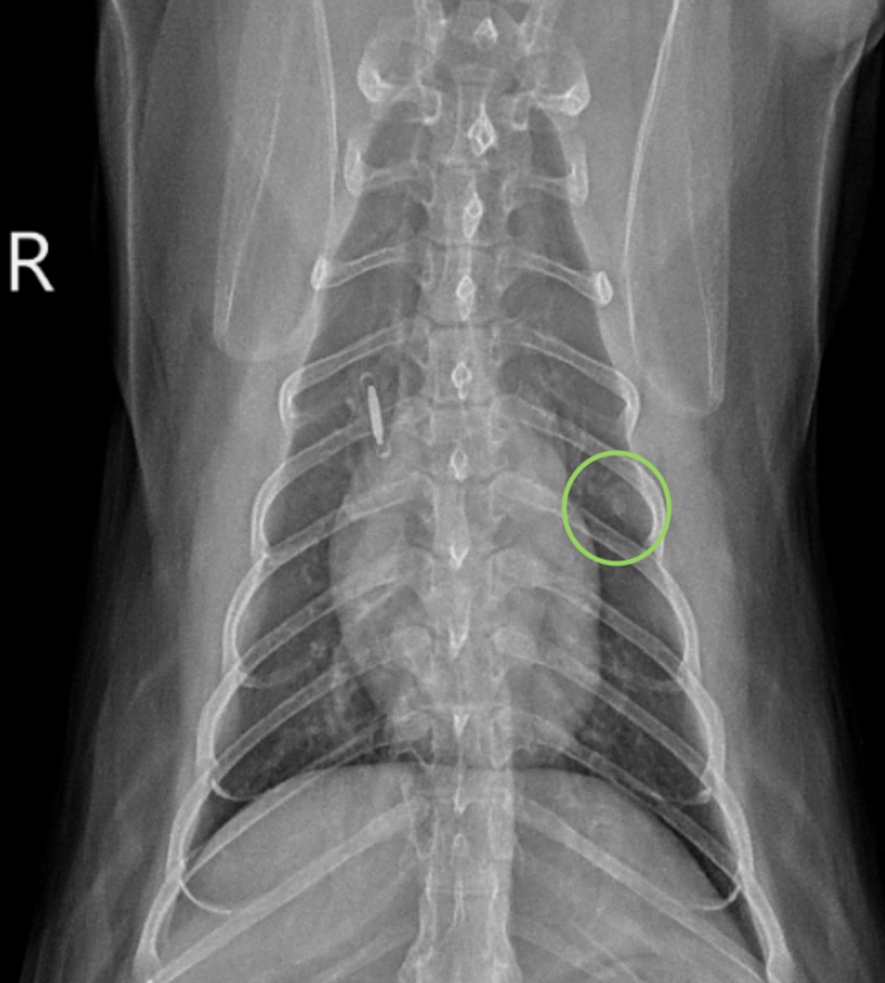
A 12-year-old male neutered domestic short hair presented for general screening prior to undergoing general anesthesia for an annual dental cleaning, and to re-evaluate a small soft tissue to mineral opaque pulmonary nodule noted in the left 5th intercostal space on thoracic radiographs obtained 5 months prior (encircled in green on the ventrodorsal view below). Differentials for the nodule included a granuloma, osteoma, or, less likely, neoplasia (metastatic vs early primary). The patient has a history of occasional vomiting secondary to presumptive chronic enteropathy and/or chronic pancreatitis, equivocal nonprogressive heart disease based on previous echocardiograms, and rare episodes of coughing. A grade II/VI left systolic heart murmur and mild periodontal disease were identified on physical exam.
DIAGNOSTICS
Routine lab work, thoracic radiographs, and abdominal ultrasound were performed. The patient was sedated for imaging.
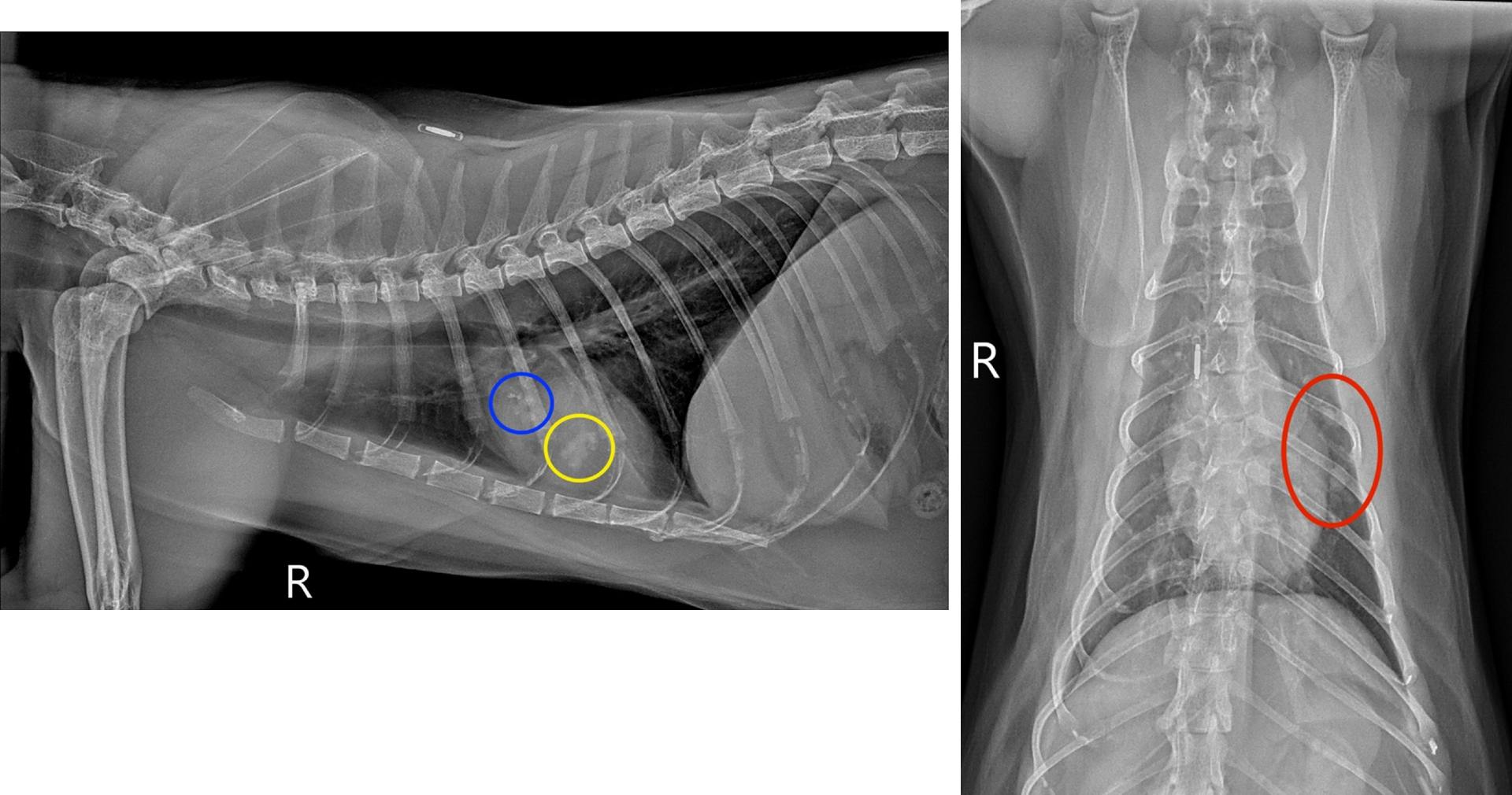
A multilobulated, mixed soft tissue and mineral opaque lesion (circled in blue) measuring 1.0 x 0.5cm is in the plane of the left cranial lung lobe on the right lateral view, partially superimposed over the 5th ribs and the heart. A second multilobulated, but primarily soft tissue opaque lesion (circled in yellow) measuring 0.6 x 0.9cm is also identified on the right lateral view, located in the 5th intercostal space caudoventral to the first described lesion. Both lesions have a linear branching and nodular appearance that creates a “tree-in-bud” pattern. On the ventrodorsal view, both lesions are in the region of the left cranial lung lobe (circled in red), which is in a similar location as the pulmonary focus seen on prior thoracic radiographs. A mild diffuse bronchial pattern was also noted.
Based on the appearance of the left cranial lung lobe lesions and concurrent mild bronchial pattern, lower airway disease (feline asthma vs chronic bronchitis), bronchial plugging, and broncholithiasis/peribronchial gland mineralization were strongly prioritized over other differentials, such as neoplasia. To further evaluate these findings a sedated, non-contrast thoracic CT was performed immediately following the radiographs.
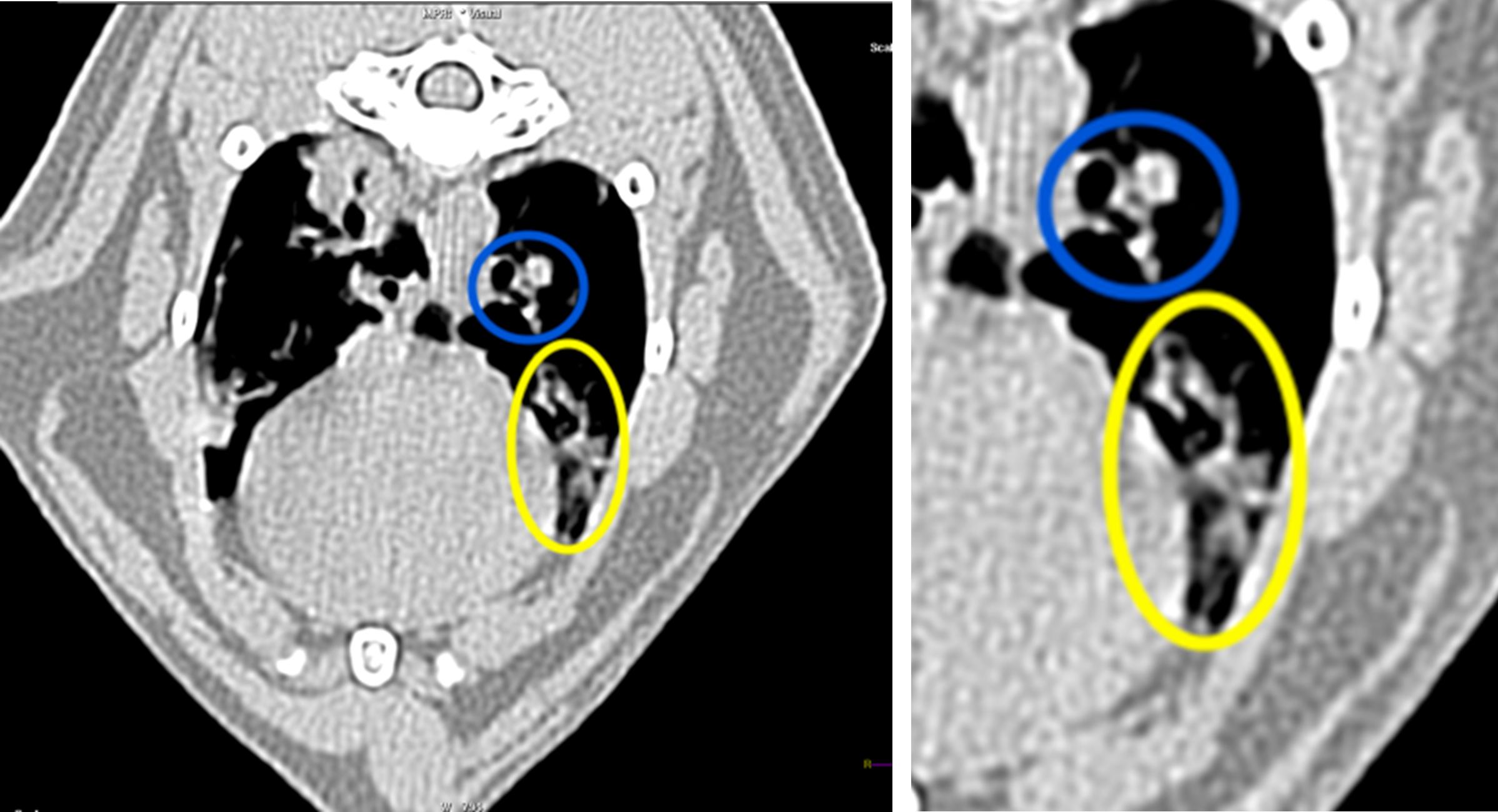
An axial CT image of the thorax is included above, along with a zoomed-in image of the area of interest. The patient’s left is to the right of the image. Several mildly dilated bronchi partially or completely filled with soft tissue attenuating material are in the left cranial lung lobe (circled in blue and yellow). The affected bronchi are branching with areas of rounded peripheral margination, creating a “tree-in-bud” appearance. The walls of these bronchi display diffuse or multifocal pinpoint hyperattenuating regions, consistent with mineralization. Additional changes not shown on the provided images include mild diffuse bronchial wall thickening throughout all lung lobes and a few smaller isolated soft tissue attenuating nodular foci associated with peripheral bronchi in other lung lobes. The isolated lesions were not seen radiographically. The patchy, soft-tissue- and gas-attenuating regions in the included right lung lobes are consistent with recumbency atelectasis and hypoinflation resulting from sedation. As suspected radiographically, lower airway disease with multilobar mucus plugging was prioritized with concurrent bronchiolithiasis/dystrophic mineralization of the peribronchial glands.
OUTCOME AND DISCUSSION
Due to a lack of current significant clinical signs associated with lower airway disease, medical management was not pursued for this patient, though follow-up imaging and close monitoring were recommended.
Thoracic radiographs are often one of the first diagnostics performed when evaluating for lower airway disease in feline patients as several radiographic changes supportive of lower airway disease have been well-documented, including bronchial pattern, lobar atelectasis due to bronchial plugging, and pulmonary hyperinflation. A “tree-in-bud” pattern has been reported in human medicine to depict the presence of small airway dilation and plugging (as with mucus or fluid). This pattern has recently been described in feline patients as an imaging feature supportive of lower airway disease. However, a “tree-in-bud” pattern has also been detected in asymptomatic feline patients or feline patients with minimal clinical signs of lower airway disease, as with the patient in this report.
The presence and severity of bronchial plugging on imaging can vary significantly and can initially present as an isolated pulmonary nodule, which can mimic pulmonary neoplasia or granuloma, as seen in the patient in this report. Given the spectrum of bronchial plugging progression and severity, it is reasonable to include bronchial plugging in the differential diagnosis of a pulmonary nodule in symptomatic or asymptomatic feline patients, especially when additional imaging findings supportive of lower airway disease are concurrently present. Thoracic CT or follow-up thoracic radiographs could then be recommended for further assessment.
Author: Raelyn Walczak, DVM, MS, DACVR
 Logo")