
Signalment:
Approximately 3 year-old female spayed Rhodesian Ridgeback
History:
Franki was out on a walk with her owner when she was shot by a hunting rifle from approximately 100 yards away. The owner immediately brought her to the local veterinarian who administered opioid analgesics and broad-spectrum antibiotics. Radiographs were obtained and sent to GCVS Surgery Service for evaluation. The wounds were flushed and a bandage placed prior to transfer for specialty care. While other hospitals recommended amputation due to the severity of the wounds, after discussion with Dr. Allen Franki’s owner elected to move forward with fracture fixation and soft tissue reconstruction.
Physical Examination:
Quiet, alert, and responsive. Large full thickness skin defect over the left distal humerus with visible avulsion injury of triceps muscle group with palpable crepitus on gentle elbow manipulation. Intact superficial pain in medial and lateral toes and well as appreciable motor function in the limb. Unable to support weight in left thoracic limb.

Figure 1

Figure 2
Figure 1 and 2: Initial wounds upon presentation prior to surgery
Diagnostics:
Humeral and elbow radiographs under general anesthesia: Traumatic and open distal spiral left humeral fracture with articular involvement in the middle of the humeral condyle. There was mild proximal displacement of the lateral condylar segment. There was also bone destruction and loss in the area of the olecranon with metal and bone fragments associated with bullet trauma.
Complete Blood Count and Biochemical Profile: Unremarkable
Thoracic Radiographs due to trauma: Unremarkable

Figure 3

Figure 4
Figure 3 and 4: Pre-operative radiographs showing degree of bone destruction and fracture configuration involving the distal humerus and joint surface
Surgical PLan:
-
-
- Reduction and stabilization of humeral fracture with type 1b external fixator
- Primary repair of triceps avulsion through bone tunnels with elbow fixed at 165 degree standing angle
- Open wound management with Vacuum Assisted Closure (V.A.C.) device at -125 mm Hg
- Axillary skin fold rotation flap for secondary closure of triceps defect after granulation tissue formation and early triceps remodeling
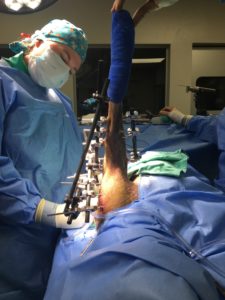
Figure 5: Intra-operative after fracture fixation with external fixator
supportive care:
-
-
-
- Continued V.A.C. therapy
- Nutritional support
- Culture and sensitivity-guided antibiotic therapy
- Multi-modal analgesic therapy
pathophysiology:
- Potential consequences of high-velocity orthopedic and soft tissue injuries include:
- Irreversible nerve damage
- Delayed tissue declaration as far out as 7 days from initial injury that leads to failure of initial repairs (e.g triceps reconstruction, skin flaps/grafts)
- Secondary/opportunistic infections that develop in necrotic tissues
- Bone sequestrum
- Progressive osteoarthritis secondary to the articular component of the injury
- Traumatic myocarditis
- Allodynia and wind-up pain if not appropriately controlled in initial post-injury period
negative pressure wound therapy:
-
-
-
-
- Therapy with V.A.C. has been shown to provide wound-healing properties in regards to:
- Antimicrobial properties via mechanical and oxygen tension properties
- Differentiation of mesenchymal cells into myofibroblasts
- Promotes cellular proliferation
- Promotes neovascularization
- Speeds up the plasmatic imbibition and inosculation phases of free graft healing
- Indications for use:
- Acute and traumatic wounds
- Chronic open wounds without active necrosis
- Skin flaps
- Meshed free grafts
- Pressure/decubital ulcers
- Contraindications
- Necrotic tissue w/out debridement
- Untreated osteomyelitis
- Exposed nerves and/or major vessels not protected with non-adherent bandage material
- Tumor malignancy
outcome:
Franki was hospitalized for 5 days after stabilization, fracture fixation, and negative pressure wound therapy. Continued open wound management was performed until reliable granulation tissue had formed and then a rotational skin flap procedure was performed and original triceps reconstruction was strengthened. External fixator was gradually deconstructed based on radiographic evidence of bone healing. Approximately 4 months from the date of injury Franki was returned to full activity.

Figure 6: Post-operative after rotational axillary skin flap

Figure 7: Franki recovering at home with one of her custom-made bandages by the amazing veterinary nursing staff

Figure 8: Franki’s leg prior to destabilization, which involves gradually removing bars and components to decrease stability and promote new bone formation

Figure 9: Franki’s leg after removal of the external fixator with an appreciable tract where one of the pins was removed

Figure 10: Franki enjoying her repaired leg as she bounds through the water!