Signalment:
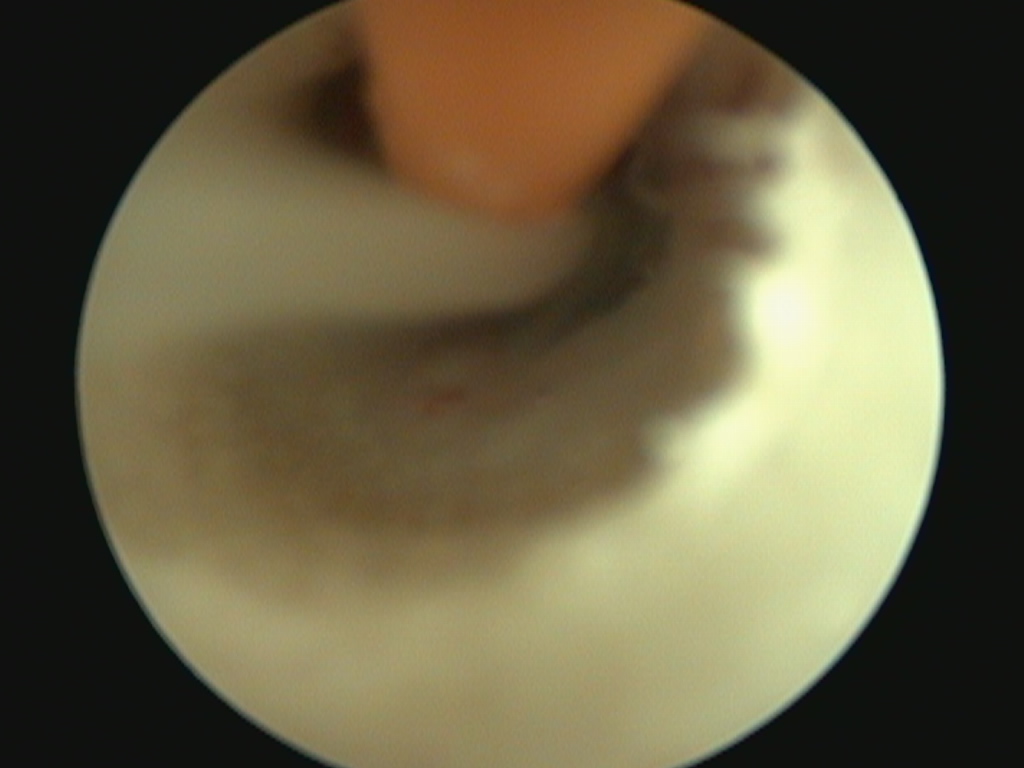
A 5mm red rubber tube is used to flush thick purulent material from the tympanic bulla using video-otoscopy
A 10-year-old Domestic Shorthair presented to GCVS Dermatology department for left-sided vestibular disease.
History:
The patient had no prior history of ear infections, but had a two-year history of nasal congestion that was responsive to corticosteroid and antibiotic injections.
The patient was initially referred to the Neurology service for evaluation of the vestibular disease. At the time of presentation, he had a two week history of ataxia and hyporrhexia. The Neurology service performed an MRI, which found fluid in both middle ears (more so in the left), and inflammation of the left external ear canal. He was diagnosed with peripheral vestibular disease, likely due to otitis media/interna, and referral to Dermatology was recommended for further diagnostics.
At the time of the Dermatology consultation, the patient had a mild left-sided head tilt and was mildly ataxic. He had been vomiting occasionally. The owner also complained of chronic sinus issues (bilateral nasal discharge, congestion, and snoring), and was concerned that this was related to his ear disease.
Physical Exam/Diagnostics:
The patient was anesthetized for video-otoscopy and deep ear flush. Myringotomy of the left ear yielded copious amount of tan, thick mucopurulent fluid. A small amount of purulent material was also found in the right tympanic bulla. Both tympanic bullae were sampled for bacterial culture and sensitivity; they were subsequently flushed with sterile saline. After consultation with Internal Medicine, a swab for an Upper Respiratory Disease RealPCR Panel was also performed to evaluate for causes of nasal congestion. The patient awoke without complications, and was sent home on a course of oral marbofloxacin pending culture results.
conclusions:
Mycoplasma infections are sensitive to marbofloxacin, therefore this was continued to control both for otitis media infection and mycoplasma disease. At the time of recheck 4 weeks later, the owner reported that the patient was doing the best he had in years, with resolution of the vestibular disease and upper respiratory signs. Aerobic bacterial culture results revealed no bacterial growth, which was a surprising finding. However, the Respiratory panel PCR was positive for Mycoplasma felis infection.
Vestibular disease can be due to central (infectious, inflammatory, or neoplastic conditions within the brain), or due to peripheral disease (otitis media/interna). Otitis media can result due to ascending infection from the nasopharynx via the Eustachian tubes, or secondary to external ear disease. In GW’s case, the lack of any history of ear disease and the positive Mycoplasma PCR would fit with an ascending infection. It is unknown at this time why the bacterial culture yielded no growth, however, prior antibiotic therapy, and the topical antimicrobial therapy instilled in the ears could be a possible explanation. It is also possible that chronic nasal and pharyngeal congestion could have decreased normal drainage from the Eustachian tubes, resulting in sterile fluid build-up in the tympanic bulla, therefore causing pressure-related vestibular disease